INM-088 key preclinical results in glaucoma
The preclinical development program for INM-088 included a number of studies comparing a number of cannabinoids, including CBN, THC and CBD, among others, to determine which cannabinoid holds the greatest potential to treat glaucoma. This preclinical research to date is comprised of both in vitro and in vivo studies and led to the selection of CBN as the lead drug candidate for further development.
The scope and results of the in vitro studies to date include the following:
1) Evaluation of the neuroprotective effects of selected cannabinoids on the differentiated retinal ganglion cells, or “RGCs”, a thin layer of neurons responsible for relaying visual signals in the eye, under normal atmospheric pressure and elevated pressure conditions. Elevated pressure mimicking high IOP had a cytotoxic effect on the RGCs. However, the combination of CBN and elevated pressure, within the same time period, resulted in a high level of cell survival in a dose dependent fashion. CBN was superior to both CBD and THC under identical testing conditions. This data indicates a potential neuroprotective effect of CBN in ocular disease.
2) Evaluation of anti-apoptotic effects of CBN on the differentiated RGCs when exposed to elevated pressure conditions. Data indicate that CBN has a significant anti-apoptotic effect on differentiated RGCs subjected to elevated pressure conditions. Exposure of RGC to high pressure for a period of 6 hours led to apoptosis ranging from 30-60%, whereas the addition of CBN resulted in a significantly higher level of cell survival.
3) Evaluation of CBN impact on the expression of specific extracellular matrix (ECM) markers on primary human trabecular meshwork (TM) cells under normal atmospheric pressure, elevated pressure and following stress-induction with Transforming Growth Factor Beta 2 (TGF-ß2), a cytokine used to alter extracellular matrix metabolism. TM cells exposed to CBN under a range of conditions, including normal pressure or elevated pressure or TGF-β2 exposure, for a duration of 72 hours, demonstrated deceased expression of protein markers associated with reduced TM outflow. These results suggest that CBN may have potential to reduce IOP through improvement in the aqueous humor outflow in the TM.
We also conducted several in vivo experiments to understand the pharmacokinetics and efficacy of CBN in the eye as a potential treatment for glaucoma. The scope of these in vivo studies to date include the following:
4) Evaluation of CBN pharmacokinetic profile in the eye and plasma of a preclinical model by direct intravitreal (IVT) injection into the eye. Following IVT delivery, systemic plasma levels of CBN were found to be below detectable limits, whereas CBN levels in the eye were shown to persist for an extended period of time with a projected half-life (t1/2) of approximately 33 hrs. These results present the prospect of high CBN localization at the site of intended treatment.
5) Evaluation of CBN neuroprotective and IOP-lowering effects in a preclinical glaucoma model by IVT injection. Biological function of the neurons was assessed through pattern electroretinogram (“pERG”) measurement of neuronal electrical activity in response to light. Results demonstrated reduced IOP and improvement of pERG function when CBN was delivered by IVT injection after episcleral laser photocoagulation.
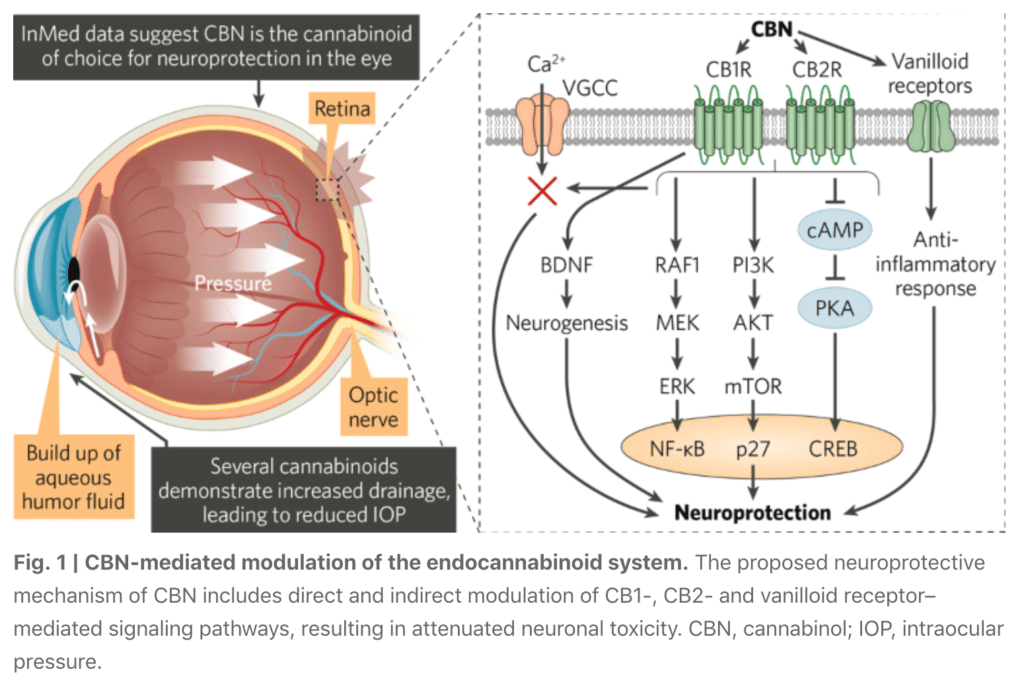
Of all the cannabinoids examined in preclinical studies, CBN demonstrated the most optimal neuroprotective effect. Furthermore, CBN also exhibited intraocular pressure reduction capability.
Current treatments for glaucoma primarily focus on decreasing fluid build-up in the eye. Our data has shown that INM-088 may provide neuroprotection in addition to modulating intraocular pressure by improving drainage of fluid in the eye.