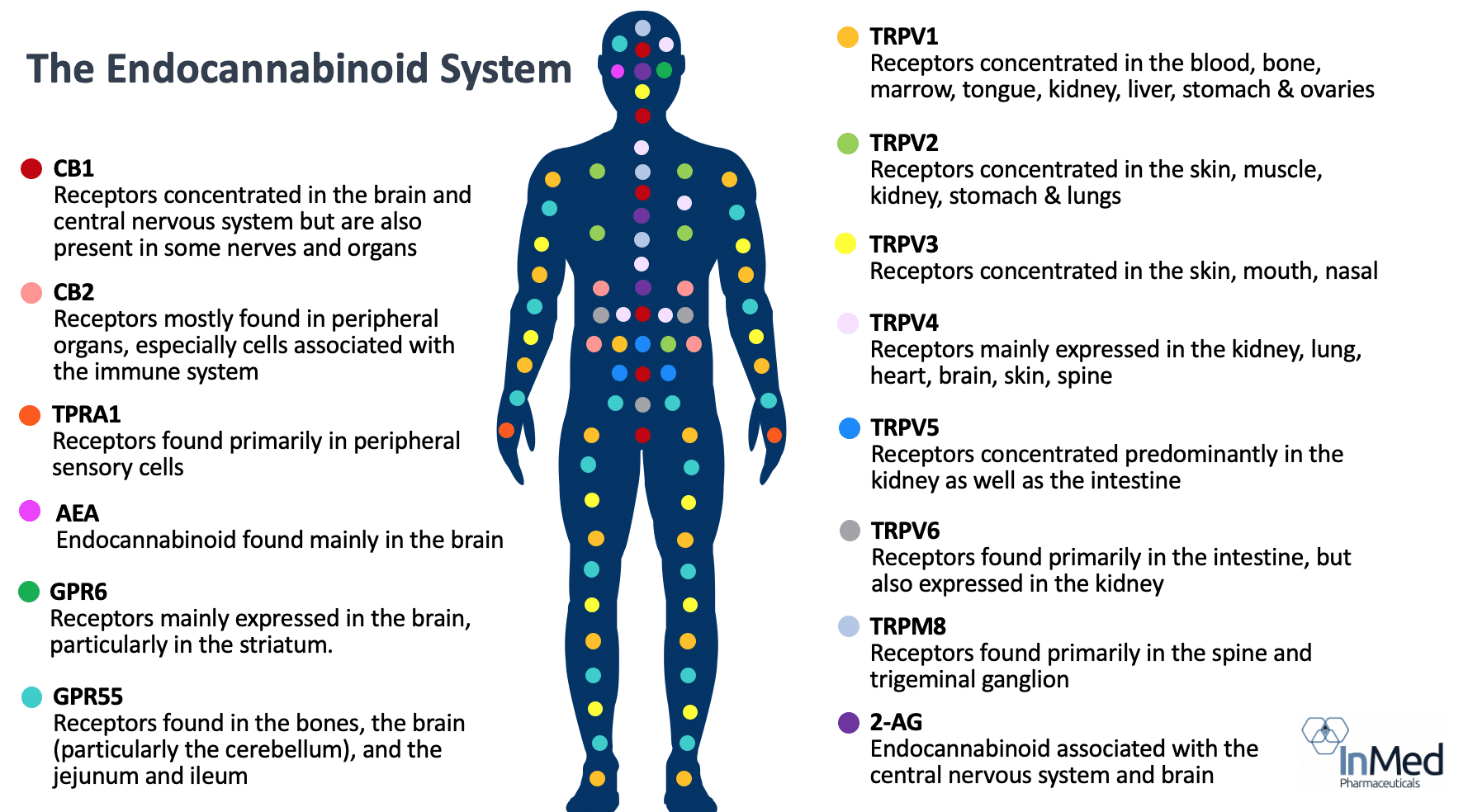
Almost every aspect of the body’s functioning involves the endocannabinoid system, such as regulating temperature, appetite, blood sugar, sleep, memory, emotional processing, pain, inflammatory and immune responses. The endocannabinoid system consists of receptors and endocannabinoids found throughout the human body including in the brain, tissues, nerves, glands, immune cells and organs, playing a critical role in maintaining homeostasis. With the important role of the endocannabinoid system on the body’s key functions, researchers have noted that “modulating endocannabinoid system activity may have therapeutic potential in almost all diseases.”
Endogenous cannabinoids, or “endocannabinoids” are naturally produced by the human body and interact with the related endocannabinoid receptor system. Exogenous, or external, cannabinoids mimic the effects and interactions of the body’s endocannabinoids. Cannabinoids act as messengers that bind to cannabinoid receptors, as well as other receptors, signaling the endocannabinoid system into action. Cannabinoid receptors are found throughout the body and are involved in brain function, immune function, pain perception and inflammation.
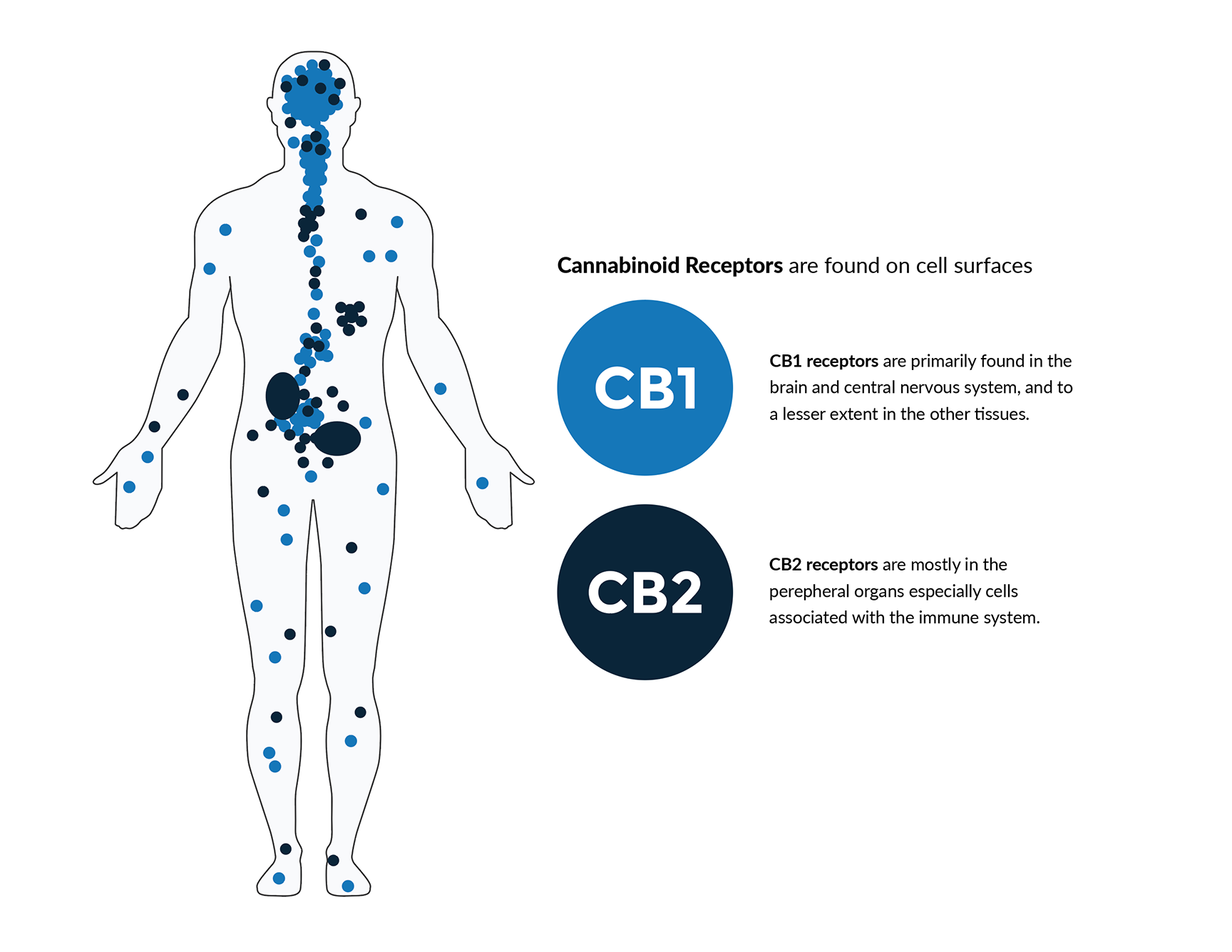
Before the 1980s, it was often speculated that cannabinoids produced their effects through nonspecific interaction with cell membranes, instead of interacting with specific receptors. The discovery of the first cannabinoid receptors occurred in the 1980s and helped to clarify their role. These receptors are common in mammals, birds, fish and reptiles. While there are numerous cannabinoid receptors in the human body, the two most well-known are the cannabinoid receptor 1 (CB1), which is more significant to the central nervous system, and cannabinoid receptor 2 (CB2), which is more common with the immune system.